 THIS BLOG POST IS NO LONGER CURRENT
THIS BLOG POST IS NO LONGER CURRENTIt's really much simpler than this.
FOR MORE RELEVANT ADVICE PLEASE CLICK THE LINK BELOW:
THIS BLOG POST IS NO LONGER CURRENT
- Dr Rupert Hinds, Feb 2010.
It's true! Five points about a disease means a whole lot to a person with good background knowledge on the subject. It's hard to explain, but a with just five points a clinician can know what do when confronted by a patient. For example a doctor may only know off the top of his head five points about cystic fibrosis...but since everything in Medicine makes sense and is logical, those five points (or concepts) connect to a vast knowledge base of medicine inside the doctor's head. It means alot. A layperson memorizing five facts (say from wikipedia) will not derive the same meaning as those facts would to a clinician.
Medicine is not all that hard. It's just about integrating concepts as they come along, and learning how to deal with people. Medicine is simple, but the devil is in the details. Textbooks will kill you. Nobody learns medicine by reading a textbook front to back. There is no alternative to experience and having a good tutor to pass on what is clinically relevant to you. The mental streams of thought used by doctors simply cannot be found in textbooks.
Dont get me wrong though. Medicine is an incredibly broad and complex field. There is just so much information to know about. They say medicine is an art... It really is. Different students approach medicine differently. Here is my approach - Ezra's approach - to studying medicine. The past three years have been spent building up background knowledge that allows me to understand, read and query authoritative sources of information (textbooks, UpToDate) quickly and efficiently. Now it's time to put what I already know to practice, and build a solid mental framework for dealing with and treating patients.
Two Broad Goals:
- To develop a framework of clinical reasoning on a sound, clinically relevant knowledge base. Understanding and familiarity without ever losing sight of the big picture.
- Notes that are simple, concise and constantly updated as I go along. Easy for revision and reference even after I graduate. Notes that "fit" nicely into clinical trains of thought ("mindlines").
Click below to read more...
Principles
- It’s all about the patient. Focus on the patient, how they present and what to do then.
- Focus only on clinically relevant material. Never getting caught up in minutae.
- Never lose sight of the BIG PICTURE and where a topic being studied lies.
- Appropriate emphasis on epidemiology – to know what is common and have a rock solid understanding of common things.
- Patient contact to integrate learnt concepts into working memory.
- Ensure topics in Case Directed Activities (Monash MBBS course material) are covered.
- Special consideration for Pharmacology.
- Think of a patient with a presenting complaint.
- Hx+Ex: What are the common things that the patient could have?
- Hx+Ex: Red flags and uncommon things that need to be ruled out.
- Ix: Confirming the diagnosis. Further investigations that are warranted.
- What are the patient issues that need to be addressed.
- Rx: Managing the patient’s condition
Knowledge ManagementThe background things that go on in my head...
1) Presenting Complaint And Differentials:
- Eg. Vomiting, cough, abdominal pain, dysuria, skin lesions etc.
- “/work/presenting complaints/*.docx” Explains how to approach a patient with a particular presenting complaint.
- “/work/presenting complaints/*.xmind” An overview (mind map) of possible diagnoses for a patient with a particular complaint.
- Appropriate emphasis will be given to red flags that need to be excluded.
- Eg. Nephrology, cardiology, pulmonology, rheumatology etc.
- A simple concise template for each clinical diagnosis will be used.
- Appropriate emphasis on epidemiology.
- “/work/diagnosis/*.docx” for each of the areas of medicine.
- Each individual diagnosis will follow a simple, straight forward template that covers clinically relevant points.
- Patient contact
- Case file review
- Rehearsed presentation on a specific differential.
What It Means In Practice
Step One: Focusing on a presenting complaint.
Hospital Experience: Ward Rounds, Consultant Tutorials, Outpatient Clinics, OHCD
“/work/presenting complaints/”
- A presenting complaint.
- Diagnostic approach.
- List differentials.
- Organize differentials by importance
- Red Flags that must be excluded
- Common Ones
- Rare/Unlikely Ones (Optional)
Step Two: Expand Each Differential
Kumar & Clark’s, Digital: Wiki/eMed/UpToDate/Harrisons
“/work/diagnosis/”
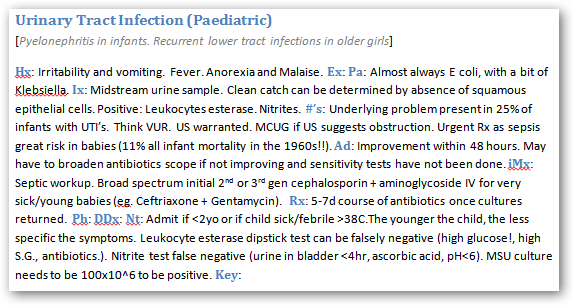
Each field has it's own document, containing many diseases. The following is a template for each individual disease.
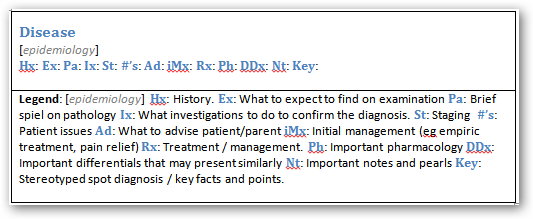
For example:
Step Three: Review
Lange Case File Series, EMQ’s For Medical Students, Kumar & Clark’s 1000 Q&A, Handbooks.
- Update “/work/presenting complaints/” with Hx and Ex pearls
- Integrate knowledge. Guidelines (eg. How to approach a febrile child)
- Do EMQ’s
- Make Sure Course Requirements Are Met (!!!). Tick off handbook.
- How does presenting complaint (eg. Vomiting) fit into the BIG PICTURE. That is, the other presenting complaints from the theme (eg. Gastroenterology).
- Be able to orate a visual Powerpoint presentation of a particular presenting complaint and it’s differentials and management. To think and to speak and elaborate without cue cards requires that information be in one’s working memory.
The Tech Behind The Scenes
Making written notes is effective, but in practice it will almost never be used for revision. Notes will be purely digital, constantly edited, reviewed, appended and revised. The goal is to make notes that I will constantly read and update as I go along. Not notes that get written then forgotten and never looked at again.
- Efficient gathering of reliable, clinically relevant information from sources such as Medscape and UpToDate. Textbooks are queried (note: not comprehensively read) for clinically relevant information as a last resort. Effectively: I will not sit down and read a book, rather, I will approach books and sources of information with a questions, and fit what I come across into my framework of reasoning.
- Mobility and freedom of access. Technology has finally progressed to a point whereby this is possible. Workstation with word/powerpoint/UpToDate has a 10hr battery life with a full sized keyboard weighs only 1.2kg.
- Goal of being as transparent as possible to allow seamless note taking that uses minimal mental effort such that more focus can be on what needs to be remembered rather than on things like text formatting.
- MS Office with an efficient use of styles to have a streamlined workflow. Presentations will be visual. No dot points. Information has to be in working memory.
- Templates for differentials.
- Redundancy by means of weekly backups to an external drive (compress work folder to “DATE.zip”. Never lose more than a week’s work, even if the computer used gets stolen or dies unexpectedly
Personally, I find Medicine quite difficult.
ReplyDeleteCheck the page at
ReplyDeletehttp://medesprogrammedicalexpert.blogspot.com/
MEDES will be a open source, non-profit programming effort to create a program which aids in diagnosis of disease. It's not a quack, not a get-rich-quick scheme, or anything like that. It's an interest in medicine and coming from my background of computer science and the fascination of a systems point of view.
Cheers,
Jukka